
From the 1Department of Rehabilitation Medicine, Hannover Medical School, 2Hannover Medical School and 3Clinic for Kidney and Hypertension Diseases, Hannover Medical School, Hanover, Germany
Background: Many patients have disabilities; it is therefore essential that medical education includes comprehensive teaching on disability and rehabilitation. In 2006, Hannover Medical School implemented an introductory course in the curriculum for medical students, on how to communicate with persons with disability and on the need for rehabilitation. The course, entitled “Introduction to medicine”, has the main goals of teaching the strategy and systematic approach of medicine to solving patients’ problems.
Methods: This paper describes the content, methods and outcomes of 1 of the 4 main themes of the “Introduction to medicine” course; the theme “Pain and disability”, which is covered in the second week of the course.
Results: Evaluation of the “Pain and disability” module found that students’ ratings for the category “patient involvement” were very high (93%), whereas their ratings for the category “examination of student knowledge” were low. The overall rating of the module was “good” (10.8 out of 15 points), but not “very good”.
Conclusion: The concept of the “Pain and disability” module is feasible and successful, even though it is scheduled early in the first year of the curriculum and approximately 350 students participate. Factors related to this success are: a mixture of teaching knowledge, supporting students’ understanding, and applying communication and physical examination skills.
Key words: teaching; medical school; persons with disabilities; undergraduate medical training; pain; disability; rehabilitation.
Accepted Jan 18, 2021; Epub ahead of print Feb 17, 2021
J Rehabil Med 2021; 53: jrm00158
Correspondence address: Christian Sturm, Department of Rehabilitation Medicine, Hannover Medical School, Hanover, Germany. E-mail: sturm.christian@mh-hannover.de
Doi: 10.2340/16501977-2797
As every medical doctor will be confronted with persons with disabilities, medical students should learn about disability and rehabilitation topics. Within a comprehensive concept of teaching disability and rehabilitation topics, in Hannover Medical School, a propaedeutic teaching course has been implemented to sensitize the students to how to communicate with persons with disability and to raise awareness about the need for rehabilitation.The survey of the students showed good acceptance of the new course, and the involvement of patients in the lessons was especially appreciated.
Disability is defined as the interaction of a person with a health condition and/or impairment and the environment (1, 2). This definition of disability includes persons with congenital conditions (e.g. cerebral palsy, spina bifida, chromosomal aberrations, etc.) and those with acquired impairments (e.g. traumatic brain injury, spinal cord injury, limb amputation, etc.). The definition also includes persons with chronic diseases, cancer, infectious diseases, and others who may experience disability related to a disease and its consequences (e.g. loss of physical performance, need for oxygen, diabetic feet, etc.). In addition, mental health disorders and learning disabilities often result in disability. For medical doctors, and other professions in medicine, education on functioning, disability and rehabilitation must be addressed in the undergraduate curriculum, since:
Medical students should therefore learn about the main factors causing disabilities, based on theoretical models, as early as possible in their education, and become competent in communicating with persons with disabilities and creating an appropriate atmosphere during conversation and examination.
Rehabilitation is one of 4 main health strategies, together with preventive, curative and supportive strategies (3–5). It is the strategy that “based on the World Health Organization’s (WHO’s) integrative model of human functioning and disability applies and integrates biomedical and engineering approaches to optimize a person’s capacity. This strategy build on and strengthen the resources of the person approaches which provide a facilitating environment. It should help to develop a person’s performance in the interaction with their environment with the goal to enable people with health conditions experiencing or likely to experience disability to achieve and maintain optimal functioning in interaction with the environment” (6). Thus, it is crucial that all physicians understand the principles of rehabilitation, the indications and contraindications for rehabilitation, rehabilitation interventions, and complex rehabilitation concepts. Based on federal regulations in Germany rehabilitation is taught together with physical medicine and naturopathy in a so-called cross-sectional field. However, the content and the academic leadership of this field in German medical faculties is very diverse (7, 8). Currently, the bodies responsible are updating the content of the curriculum (with rehabilitation as an independent field of learning in the course examination) and introducing more rehabilitation topics into the catalogue of learning goals (9).
Hannover Medical School has implemented a teaching course to impart basic knowledge about disability and rehabilitation, teach medical students to how to communicate with persons with disability, and raise awareness of the need for rehabilitation. This course is integrated into the initial teaching block on the principles of clinical work (the so-called Propädeutikum), which is delivered at the start of the first year medical student curriculum (10). The course has the following teaching/learning goals:
Model curriculum for medicine at Hannover Medical School
In 2006, Hannover Medical School established a model curriculum for medical education. Its main goal is to prepare students for independent clinical work. The curriculum dissolved the previously used strict differentiation of theoretical fields (physics, chemistry, anatomy, physiology, etc.) and clinical areas (internal medicine, surgery, etc.). The 6-year curriculum includes 3 courses focusing on the following general clinical principles or principles of a physician’s work:
The sixth year of the curriculum is dedicated to practical clinical training (as in all German medical schools).
A further characteristic of the model curriculum is that the clinical fields are organized into blocks of 1 or 2 weeks, in which theoretical knowledge and practical skills are taught on a whole-day basis, ending with an practical examination course . Based on the modell curriculum the above-mentioned course on “Rehabilitation, physical medicine and naturopathy” is 2 weeks long and is provided in the fifth year (11).
“Introduction to medicine” course
The “Introduction to medicine” course (Latin: Propaedeuticum) is the initial course of the Hannover Medical School curriculum. Its main goals are to teach understanding of the strategy and systematic approach of medicine to solving patient’s problems. The course illustrates the pathway, from taking a medical history and physical examination, through the process of preliminary clinical diagnosis, diagnostic measures, such as imaging or laboratory analysis, to confirm or differentiate the diagnosis, to treatment planning and rehabilitation measures (Fig. 1). In addition, the course illustrates why theoretical and clinical knowledge is important in this process, based on knowledge of the body and its functions, patho-mechanisms, diseases, treatment strategies, and psychosocial aspects of patients and their health conditions. The course also reflects on the role models of physicians, and introduces the first stages of clinical investigation and the principles of how to communicate with patients.
The “Introduction to medicine” course comprises 4 teaching blocks, of one week each, comprising lectures, seminars and practical workshops. Each block has a main theme and is led by 1 or 2 specialists in the respective field. Lectures and seminars are given by specialized lecturers, resulting in a highly interdisciplinary faculty. Practical workshops are partially run by student tutors, because it has been shown that students prefer learning professionalism in near-peer-led lessons (12). The starting points for clinical and theoretical lectures are patient interviews performed by the lecturers in front of the students.
The themes of the 4 weeks are as follows:
In addition, all students participate in clinical ward rounds in different clinical departments. These teaching rounds are led by experienced senior doctors, and focus on how to approach patients in a professional way, how to systematically analyse patients’ problems, and how to make decisions on further diagnostics and treatment.
The objective of this paper is to describe the content, methods and outcomes of the theme “Pain and disability”, which is provided as the second week of the “Introduction to medicine” course.
Fig. 1. Scheme for the topic “From the patient’s problems to diagnosis, treatment, and rehabilitation”.
Learning goals and themes
The teaching block on pain and disability includes the application of knowledge, understanding mechanisms, competencies and clinical skills. The teaching/learning goals are as follows:
○ Symptoms of low back pain and how to differentiate them in taking a history and physical examination.
○ Interrelation of symptoms with anatomical structures and the patho-mechanism of lumbar disc herniation.
○ Role of imaging in diagnosing low back pain.
○ Treatment options (pharmacology, surgery, and physical medicine).
○ Understanding psychosocial factors related to low back pain.
Pain as a symptom and/or disease:
○ Understanding the role of pain as a symptom and as disease, and basic knowledge about pain perception.
○ Understanding the International Classification of Functioning, Disability and Health (ICF) and applying it to the problems of persons with health conditions.
○ Understanding functioning and disability in patients with spinal cord injury
○ Understanding the WHO definition of disability.
○ Raising awareness of patient-adapted communication in order to build an appropriate atmosphere for medical treatment.
○ Reflecting on how to communicate with persons with disabilities.
○ First steps in examination techniques for the spine and cranio-mandibular joint, and practicing first steps in patient interviews.
○ Self-reflection on the examination of peers and on being examined.
Timetable and teaching elements
Each day of the teaching week has a topic, as illustrated in Table I. Learning goals are presented to the students each day. Patient interviews between the teacher and a single patient at a time and lectures for all students are held in the morning. Practical workshops (examination of the spine: first steps) and seminars (patient interviews) are run in smaller groups in the afternoon. In addition, each student has to complete homework, consisting of applying a simple ICF-based questionnaire to a person with a disease or health condition (in a 1-to-1 interview). To allow enough time for students to perform the homework, the ICF model and the questionnaire are introduced in the previous week.
The teaching units are related to the teaching goals as follows:
○ Patient interview in the lecture hall, lecture about epidemiology and differentiation of low back pain.
○ Lectures on lumbar disc herniation and surgical interventions.
○ Lectures on differential diagnosis of low back pain and psychosocial factors associated with low back pain.
○ Lectures on principles of pain medicine and introduction to neurophysiological mechanisms of pain perception.
○ Lectures about principles of pharmacotherapy and physical therapy for pain.
○ Lecture on definitions and relevance of disability and functioning.
○ Interviews with patients with spinal cord injury, focusing on aspects of activities, participation, and relevant contextual factors.
○ Lecture on the principles of rehabilitation.
○ Lecture on clinical examination and practicing first steps of examination of the spine and the cranio-mandibular joint in groups of 6–8 students (including documentation of findings).
○ Lecture on communication with persons with disabilities, given by a student who is a wheelchair user.
○ Seminars of 15–20 students to practice patient interviews with a so-called “actor patient”.
○ Homework of a 1-to-1 interview with a person of choice (e.g. a family member) on the impact of a disease on body functions, activities and participation, and the most relevant environmental factors (using a short ICF-based questionnaire with 15 items and the possibility of free-text answers and comments on the questionnaire itself).
○ Interactive lectures on the results of the homework and self-reflection on the examination of peers as well as being examined.
A specific feature of the “Pain and disability” module is the strong active involvement of the students in the learning/teaching activities. These include:
Because of the complexity of the teaching block, the academic leading the teaching week is continuously present in the lecture hall and introduces every lecture. They explain the teaching goals and, if necessary, discuss inconsistencies in the content and provide additional explanation.
The questionnaire for the individual patient interviews contains 15 questions out of the ICF chapters “Body functions”, “Activities and Participation” and “Environmental factors”. The answers have tick boxes with the scores “no problem”, “mild problem” and “severe problem”, in addition to “barrier” or “facilitator”, respectively. In addition, students can add more dimensions in a free-text box if they consider it necessary. At the end of the questionnaire the student can comment on the relevance of the questionnaire for the interview and on the feasibility of use of the tool. These comments also are subject to discussion on the questionnaire on the final day of the week.
On Monday of the following week the students undergo a written examination with 30 multiple-choice questions (1 correct answer out of 5 choices). The examination covers facts from the lectures, and clinical decision-making based on a theoretical paper case (i.e. diagnosis, imaging, treatment decision, follow-up). Due to lack of personnel there is no skill-based practical exam. Documentation of the clinical examination between students in small groups must be signed-off by the mentor, and the homework is completed under controlled conditions (both documents are completed in the university’s student’s teaching portal). After the written examination, the students evaluate the quality of the course, using Hannover Medical School’s standardized evaluation questionnaire (13, 14).
In order to help students prepare for the examination, second year students offer tutorials on Friday afternoon. Although participation in the tutorials is voluntary, two-thirds of students choose to participate. For foreign students, a specific supportive programme is offered, comprising introductory seminars, help with specific terminology, and continuous tutorials throughout the first year. The main effect is more time for introductions, and division of the (approximately 30) students into smaller groups, each of whom is assigned a tutor. A fixed contact person is made available within this support programme to discuss any problems that arise.
Table I. Timetable for the thematic week “Pain and disability”
A total of 270–290 medical students and 70–80 dentistry students participate in the “Pain and disability” module of the “Introduction to medicine” course each year. However, the examination is for medical students only; dentistry students are examined separately according to state regulations. Knowledge is examined via a multiple-choice examination (via a laptop-based central examination system). Evaluation of the examination scores (Fig. 2) reveals that 97% of students pass and the range of scores is well distributed.
Clinical and psycho-social skills are not examined; however, discussion with students and lecturers’ feedback from the seminars and workshops provide some evidence that the teaching/learning goals in this sector are also achieved.
Fig. 2. Results of the written examination (distribution of scores for 2019).
The homework is mandatory for certification of the course, and (with very few exceptions) all students completed the online questionnaire. Over the years the results have been highly homogenous. However, analysis of the free-text answers reveals that some misunderstandings occur regarding the application of ICF terms. These misunderstandings are discussed in the final lecture of the week in combination with the demonstration of 3–4 selected results.
The results of students’ ratings on the quality of the “Pain and disability” module are summarized in Fig. 3. The evaluation rating scale is: 15–13 points = 1, 12–10 points = 2, 9–7 points = 3, 6–4 points = 4, 3–1 points = 5, 0 points = 6. Ratings for the category “patient involvement” are very high (93%), whereas ratings for the “examination” are low. This can be explained by the perceived difficulty of the examination, which has a higher level of difficulty than the examination in the previous week. In general, students rate the courses lower when the difficulty of the examination is higher than they had prepared for (15). Other investigation reports that there is a significant correlation between evaluation and the examination grades (16). In this week, which has a practical focus, some content must be learned independently in a short period of time. This may explain why the overall rating of the course was “good” (10.8 out of 15 points), and not “very good”
The free-text answers reveal some points that the students regarded very positively, e.g. the involvement of patients and the opportunity to practise patient interviews. On the other hand, the students regarded some of the questions in the examination as too detailed.
Fig. 3. Student’s ratings on the quality of the “Pain and disability” module. Exam: examination; pts.: points.
Many publications emphasize that knowledge and understanding of disability and rehabilitation among medical school graduates is lacking (17). This includes significant uncertainties among graduates regarding communication with persons with disabilities, and their societal attitudes (18). Other papers stress the importance of acquiring knowledge of rehabilitation medicine (19–22). To close these gaps, several proposals have been published regarding implementation of topics on disability and rehabilitation medicine in undergraduate medical training (23–29).
Gutenbrunner et al. published a comprehensive concept of how to implement disability and rehabilitation topics in undergraduate medical training (11). This concept includes a multistep approach with repeated courses (or single lectures and seminars) throughout the 6 years of medical study. It starts with the introductory (propaedeutic) course discussed here, and continues in the second and third years with lectures and examination skills training. In the fifth year a 2-week block on “Physical and rehabilitation medicine”, delivered via lectures, seminars and practical workshops, is mandatory for all students. In addition, the students can choose elective clinical training in the Department of Rehabilitation Medicine. This demonstrates that the thematic week on “Pain and disability” in the “Introduction to medicine” course, described here, is not an isolated teaching element, but part of a more comprehensive teaching concept.
Another line of integration is the other thematic weeks and the ward teaching units. In addition to the above-mentioned topics, the following skills were taught: reflection on the role of the physician, patient interviews, informing patients about “bad news”, clinical examination skills (e.g. breast, lung), etc.
This paper shows that the concept of the course “Introduction to medicine”, including the theme “Pain and disability”, is a feasible and successful approach, even though it is scheduled early in the curriculum (the second week of the first year) and approximately 350 students participate. Factors related to the success of this course are the mixture of teaching knowledge, supporting understanding, and applying communication and physical examination skills. The starting point, with real patients, is another factor that creates an atmosphere of attention and supports the students’ feeling of relevance. The practical courses, as well as the homework, also contribute to the high motivation of the students.
There is a strong consensus in the literature that physicians must acquire a broad spectrum of knowledge and skill, and develop a professional attitude (30). The course on “Introduction to medicine” at Hannover Medical School has only introductory (propaedeutic) scope; the most important levels of learning are addressed (learning some facts of anatomy, pathology and disease symptoms, understanding of interrelations (e.g. between anatomical structures, pathologies and symptoms), examination skills and, perhaps most important, experiencing direct contact with patients). The authors expect that these experiences will induce some self-reflection with longer-lasting effects; although the long-term effects of the course have not yet been evaluated, reports from graduates indicate that this might be the case. However, these effects must be further elucidated in future studies.
Based on our observations, the following factors are key to the positive effects of the “Pain and disability” module described here:
A high level of effort is required of the organizers to deliver such a complex module with a wide spectrum of teaching approaches and strong active involvement of the students, including many different departments. However, the very high motivation of the students observed, with high level of involvement in the discussion phases of the lectures and very positive feedback, indicate that this effort is worthwhile.
The concept also has some weaknesses; some of which are inherent, and some may be reduced by the continuous process of quality improvement related to the students’ evaluation. Some students state that the content is too advanced and the course should be scheduled later in the curriculum. It also has been reported that the course is too complex and the learning goals too broad. On the other hand, the students are very positive about the content and, in particular, are interested in the patient demonstrations, the practical learning, and the way the course is moderated.
The authors do not know of the existence of any similar teaching modules. In most cases the issue of disability is introduced at the end of medical studies, or is not included at all. Further studies are necessary to determine if this knowledge and understanding differs from that of cohorts in other medical faculties.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize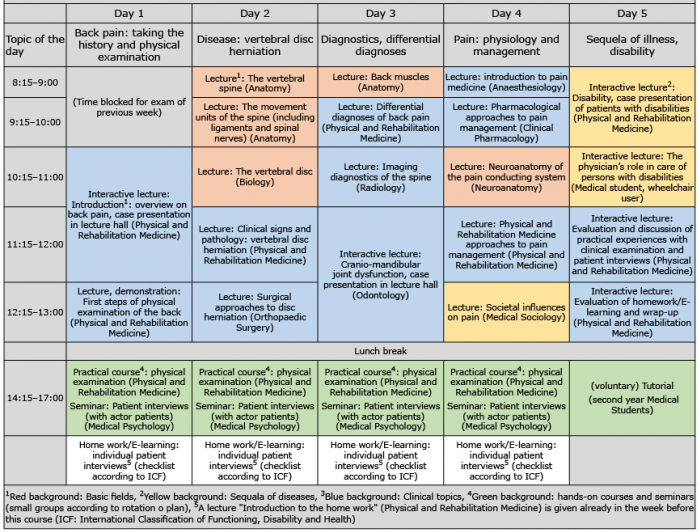 Click to show fullsize
Click to show fullsize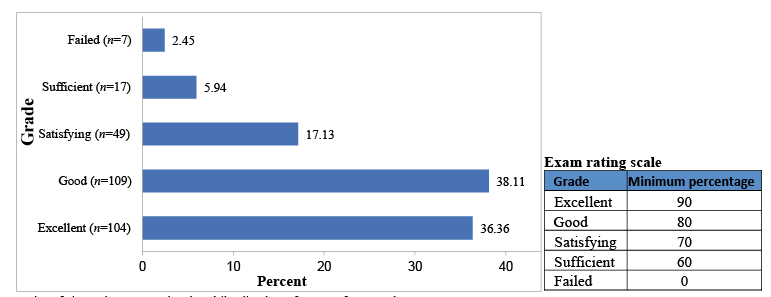 Click to show fullsize
Click to show fullsize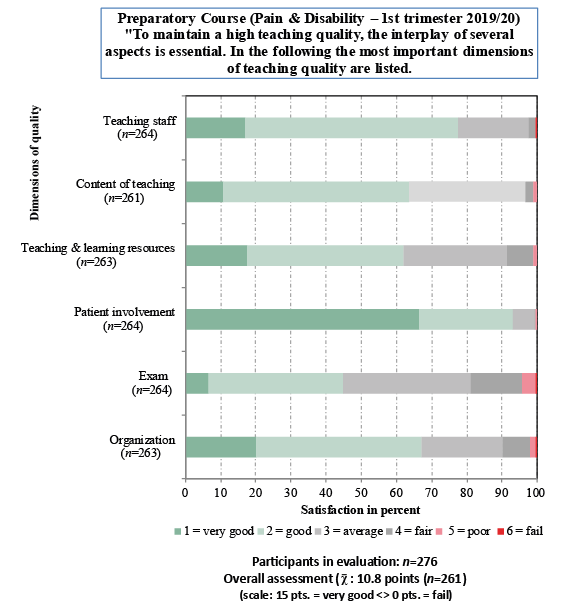 Click to show fullsize
Click to show fullsize